Vitamin Spotlight: Folate
Folate, also known as vitamin B9, is a water soluble vitamin. It has many important functions in the body, including: 1) synthesis of nucleic acids (for DNA production and repair and tRNA); 2) participation in single carbon metabolism/methylation and homocysteine regulation; 3) interconversion of amino acids (for neurotransmitter production and detoxification); and 4) formation and maturation of red and white blood cells and platelet production. Folate works synergistically with several of the other B vitamins, in particular B2, B6 and B12, which aid in its metabolic functions (Higdon, 2014).
There are over 150 different forms of folate that are naturally occurring in plants. By contrast, folic acid is the man-made, synthetic form of folate. While most forms of plant folate are in reduced forms (Witthöft et al., 1999), folic acid must go through a significant transformation before the body can utilize it:
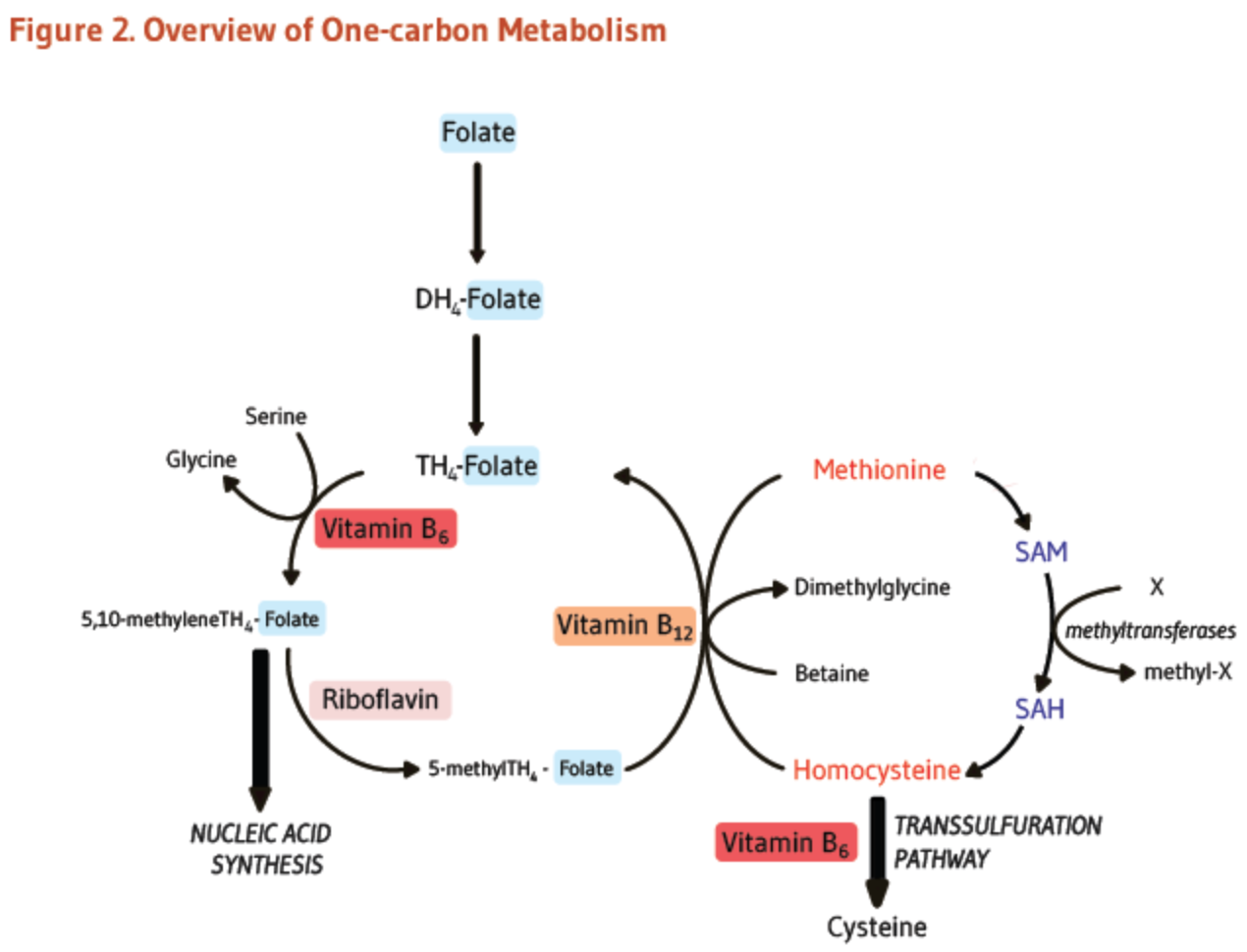
Reference: Bailey & Gregory, 1999.
As the above diagram illustrates, folic acid must first be converted to dihydrofolate (DH4), then to tetrahydrofolate (TH4), and then further converted to folinic acid (5,10-methyleneTH4, which may be used for DNA bases) or methylfolate (5-methylTH4, needed for DNA methylation) before it can be used.
In 1998, the U.S. FDA mandated that all processed grain products be fortified with 140 μg of folic acid (for every 100g of product) in order to stem the growing number of neural tube defects (Nix, 2017). While neural tube defects have declined since this time period, emerging research suggests that this extensive fortification may have some negative health consequences. Folic acid is both more bioavailable than natural folate (Nix, 2017), and preferentially binds to the folate receptor (Henderson, 1990). As folic acid is more difficult for the body to metabolize, this may result in large quantities of unmetabolized folic acid (“UMFA”) in the blood (Bailey & Ayling, 2009). One study found that an intake of greater than 200 μg of folic acid led to the accumulation of UMFA in the blood (Crider et al., 2011). As Nix notes, highly enriched cereal alone may provide 400 μg or more folic acid per serving (Nix, 2017, p. 101). Therefore, Americans on a high-processed carbohydrate diet, may be getting physiological doses of folic acid from their food supply, which may be contributing to high levels of UMFA.
The research on folic acid and UMFA is rapidly emerging. While it may be premature to draw conclusions at this early stage, studies have associated folic acid with the development of certain cancers. For example, a randomized, controlled trial found that men taking 1mg of folic acid daily had an increased risk of developing prostate cancer (Figueiredo et al., 2009). Another study has associated the folic acid fortification program in Chile with an increase in the rate of colon cancer (Hirsch et al., 2009). Other studies have been done to assess the impact of UMFA in the body. For example, one study has associated UMFA with a reduction in natural killer cells (Troen et al., 2006). A study in Ireland identified that the bulk of the senior population had high levels of UMFA. Upon concerns that this may have been masking B12 deficiencies, and contributing to cancer acceleration, Ireland has since abandoned its folic acid fortification program (Boilson et al., 2012). Interestingly, most European countries never adopted folic acid fortification in the first place, and I personally believe this is one area where we may see legislative changes in other countries in the future, as the research continues to emerge.
Folate is a perfect example of the role that biochemical individuality, life-cycle and lifestyle factors may play in determining nutrition needs, including the potential need for supplementation. As we have seen, the metabolism of folate is complex and requires: 1) an uncooked, natural source of folate; 2) functioning enzymes; 3) available receptors; 4) transport into the cell; and 5) B2, B6, B12. All of these factors must be taken into consideration when evaluating nutrition and supplementation needs.
First, there are many genetic variations that may impact an individual’s folate requirements. Individuals may carry polymorphisms in the genes that code for the enzymes responsible for folate metabolism (e.g., DHFR, SHMT & MTHFR). This may further impact the body’s ability to convert folic acid and any non-reduced folates from foods to the active forms of folate. For example, the MTHFR C677T genetic polymorphism is very common. Individuals with this polymorphism have a 30-65% reduced function of the MTHFR enzyme, depending upon whether they carry one or two copies of this gene (Higdon, 2014). This genetic polymorphism is associated with the development of cardiovascular disease, thrombolism, thyroid disease, and recurrent miscarriage. One example of this relates to homocysteine regulation. Without enough methylfolate to participate in the methylation cycle, homocysteine can not be properly recycled (Nix, 2017). High homocysteine can damage endothelial cells, and has been associated with the development of cardiovascular disease (Maron & Loscalzo, 2009). As a result, individuals with polymorphisms in the genes that encode for folate cycle enzymes may have an increased need for folate in the diet, and should avoid supplementation with folic acid for the reasons discussed above. Individuals with these polymorphisms may further need to supplement with active folates to ensure that they are meeting their functional needs.
Second, the need for dietary folate may vary throughout the life cycle. Because of its role in DNA synthesis, folate has been shown to be extremely important during pregnancy, in particular in preventing neural tube defects (which usually occur in the first 28 days of gestation)(Nix, 2017). Folate is also important for growth, and therefore children and adolescents may need higher levels of folate, as folate deficiencies may negatively impact growth (Nix, 2017).
Third, lifestyle factors, such as the amount of raw, leafy greens one consumes, may influence supplementation needs. Cooking, food processing, and storage significantly reduce folate content by 50-90% (Nix, 2017).
Therefore, if an individual is not consuming raw leafy greens or green juice (or other uncooked sources of folate), it may be advisable to supplement. By contrast, as noted above, an individual who consumes large quantities of grain-based processed foods, may be consuming excessive amounts of folic acid. Further, studies have indicated that alcohol and smoking both negatively impact folate status (Baron et al., 1998). These lifestyle factors should be taken into consideration when evaluating folate needs.
The current folate DRI for adults is 400 μg DFE per day, with the adult UL of 1000 μg per day (Nix, 2017). Due to the above biochemical, life-cycle and lifestyle factors, an appropriate level of supplementation is going to be very specific to the individual.
References:
Baron, J. A., Sandler, R. S., Haile, R. W., Mandel, J. S., Mott, L. A., & Greenberg, E. R. (1998). Folate intake, alcohol consumption, cigarette smoking, and risk of colorectal adenomas. Journal of the National Cancer Institute, 90(1), 57-62.
Bailey, S. W., & Ayling, J. E. (2009). The extremely slow and variable activity of dihydrofolate reductase in human liver and its implications for high folic acid intake. Proceedings of the National Academy of Sciences, 106(36), 15424-15429.
Bailey, L. B., & Gregory III, J. F. (1999). Folate metabolism and requirements. The Journal of nutrition, 129(4), 779-782.
Boilson, A., Staines, A., Kelleher, C. C., Daly, L., Shirley, I., Shrivastava, A., ... & MacCooey, A. (2012). Unmetabolized folic acid prevalence is widespread in the older Irish population despite the lack of a mandatory fortification program. The American Journal of Clinical Nutrition, 96(3), 613-621.
Crider, K. S., Bailey, L. B., & Berry, R. J. (2011). Folic acid food fortification—its history, effect, concerns, and future directions. Nutrients, 3(3), 370-384.
Figueiredo, J. C., Grau, M. V., Haile, R. W., Sandler, R. S., Summers, R. W., Bresalier, R. S., ... & Baron, J. A. (2009). Folic acid and risk of prostate cancer: results from a randomized clinical trial. Journal of the National Cancer Institute, 101(6), 432-435.
Henderson, G. B. (1990). Folate-binding proteins. Annual review of nutrition, 10(1), 319-335.
Higdon, J. Linus Pauling Institute. (2014). Folate. Retrieved from http://lpi.oregonstate.edu/mic/vitamins/folate#cardiovascular-disease-prevention
Hirsch, S., Sanchez, H., Albala, C., de la Maza, M. P., Barrera, G., Leiva, L., & Bunout, D. (2009). Colon cancer in Chile before and after the start of the flour fortification program with folic acid. European journal of gastroenterology & hepatology, 21(4), 346-349.
Maron, B. A., & Loscalzo, J. (2009). The treatment of hyperhomocysteinemia. Annual review of medicine, 60, 39-54.
Nix, S. (2017). Williams' basic nutrition & diet therapy (15th ed.). Chapter 6. St. Louis, MO: Elsevier.
Troen, A. M., Mitchell, B., Sorensen, B., Wener, M. H., Johnston, A., Wood, B., ... & Potter, J. D. (2006). Unmetabolized folic acid in plasma is associated with reduced natural killer cell cytotoxicity among postmenopausal women. The Journal of nutrition, 136(1), 189-194.
Witthöft, C. M., Forssén, K., Johannesson, L., & Jägerstad, M. (1999). Folates-food sources, analyses, retention and bioavailability. Näringsforskning, 43(1), 138-146.